Website updated (from 1st January 2022)
This website has been updated, by the inclusion of additional ultrasound sequences of both breastfeeding & bottle-feeding. 'SimpleSite' has a linear design, which means you need to keep scrolling down to see content!
CONTENT:
1. Additional sequences of breastfeeding are all referred to in an accompanying draft manuscript, being prepared for publication (constructive comments welcome). Appended is a longer narrative description of the contents of these videos. [This series of ultrasound tudies was funded by Philips Research, Eindhoven.]
2. Also uploaded are ultrasound sequences of bottle-feeding, by previously exclusively breast-fed babies; requested by users of this site. [This series of bottle-feeding studies was funded by Lansinoh (UK).]
The accompanying document represents the 'Final Report' to the funders (accessible on their website) - the views expressed within the Final Report remain solely those of the authors, and do not necessarily reflect those of the funders.
Timeline: Modifications commenced: 24th Dec 2021; uploading process incomplete as of this date (2nd January 2022).
Below these recent ultrasound recordings, can be found three landmark, archival imaging studies: Ardran et al, 1958a & b; Eishima, 1991; & Weber et al, 1986 - none of which has previously been available.
Research studies into breastfeeding
THIS SITE CONTAINS PREVIOUSLY UNPUBLISHED RESEARCH STUDIES (including ULTRASOUND), AS WELL AS ARCHIVAL IMAGING STUDIES OF BREAST- & BOTTLE-FEEDING. Please feel free to post questions relating to its content.
Schematic to aid understanding of more recent ultrasound scans
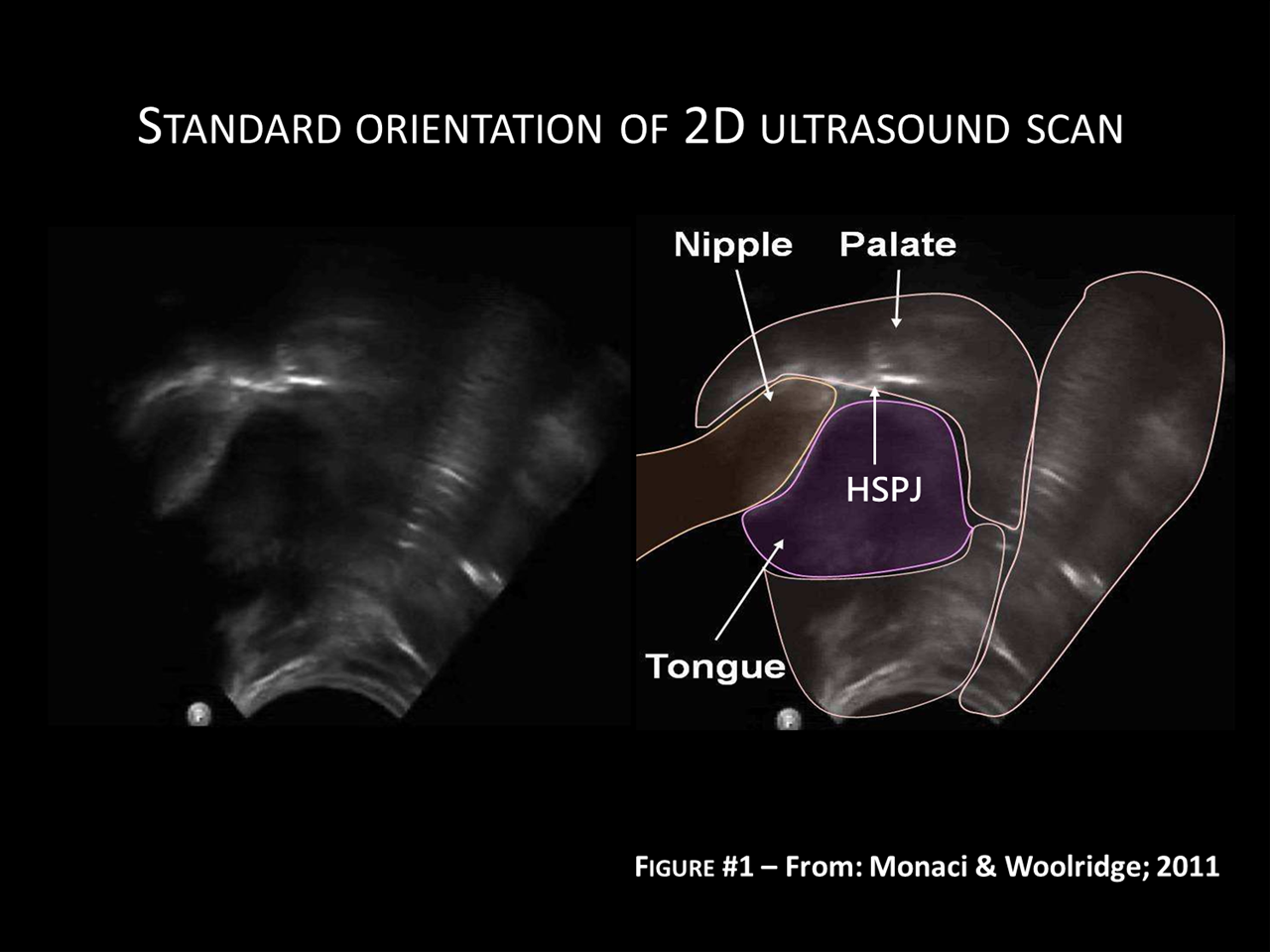
The figure below (Schematic Fig. 1) shows a schematic overlay of the ultrasound scans, which should help to explain what can be seen in the ultrasound videos below.
In all cases the breast/nipple enters the baby's mouth from the left (but it can only be viewed behind the shadow cast by the lower jaw).
The tongue is applied to the underside of the breast/nipple and, dynamically, a wave sweeps from left to right, from the front of the mouth, towards the back of the oral cavity (gullet).
The palate is viewed as two different interfaces: the hard palate (front half of mouth) is seen as a solid white line, lying above and against the nipple. The soft palate (rear half of the mouth) can only be seen where it interfaces with air in the nasal cavity (i.e. the back of soft palate). The transition between the front face of the hard palate, and the rear face of the soft palate, is known as the Hard-Soft Palate Junction (HSPJ). The interface between the soft palate and the tongue cannot easily be seen, because both are soft tissues with no air in between.
Video #1: NORMAL suckling - half normal speed, 21s duration - mixture of pure peristalsis, with intermittent 'added suction' elements.
This sequence of normal suckling comprises 36 sucks - 28 are almost solely peristaltic, while 8 also show 'added localised depression' of the tongue surface. There are also 8 swallows in this sequence which are linked in time with the extractive tongue movements.
Video #2: U/s showing baby using anterior of tongue to squeeze milk from ducts within the nipple.
The baby is using wave-like tongue compression of the ANTERIOR section of the tongue, applied to the underside of the nipple. Milk within the ducts (dark) is squeezed ahead by the wave, although this baby is appears to be using this action to 'gate' outflow of milk from the nipple.
Video #3: Milk bolus being swept to rear of oral cavity - one quarter of normal speed, 14s duration. [Image can be enlarged to full screen, by clicking button at bottom right]
The milk bolus, collected at the nipple tip, is swept over the rear surface of the tongue by peristalsis. It passes under the soft palate, before entering the oro-pharyngeal space (gullet); here it may be swallowed, or pool at the sides until there is sufficient to swallow.
Video #4: U/s sequence showing the baby employ 'localised added suction' (identified by Eishima, 1991; & Geddes et al, 2008)
Evidence from this U/s is that milk is flowing well, shown by an enlarging 'dark' space at the nipple tip, with few reflective particles. At other times, there are bursts of highly reflective particles; these suggest that CO2 is being pulled out of solution by high suction pressure ('Cavitation').
Video #6: Evidence that 'added suction' may helpt to refill teat.
This U/s sequence suggsts that while 'added suction' is usually localised at the nipple tip, it can appear more anteriorly where it seems to aid refilling of the ducts within the teat, from milk within the breast.
This document contains an extended narrative description of each of the videos shown above.
Video #7A: The next five sequences are all from the same baby; she had been exclusively breast-fed to 15 weeks, with bottles of EBM only recently having been introduced.
The bottle teat is clearly visualised by two double echoes, two from the rear wall of the teat and two from the near wall. The key feature in this sequence is wave-like compression of bottle teat in ANTERIOR of the baby's mouth.
Video #7B: U/s sequence showing how 'added suction' causes abnormal distortion of soft palate.
This U/s sequence (just 30 sec later) focuses on the soft palate. The 'localised added suction', created by the baby, can't extend the bottle teat further into the mouth, because it won't stretch. Instead the soft palate is pulled further forward; it distorts so much that it hits the teat tip.
Video #7C: Slow motion showing collisions between soft palate and bottle teat tip.
This U/s sequence comprises 37 sucks, with the soft palate colliding with the bottle teat tip on 11-12 occasions; i.e. once every 4 sucks.
Video #7D: Same baby as in #7A-#7C, now being breast-fed.
Same baby as in previous sequences, now being breast-fed. Uniquely for a breast-fed baby (not previously recorded), we see the same collisions between the soft palate and the nipple tip. We are unable to say whether this occurred before bottle-feeds were introduced.
The Biomechanics of Breastfeeding: Bridging the gap between engineering-based studies and clinical practice.
Here is my personal copy of the manuscript: "The Biomechanics of Breastfeeding: Bridging the gap between engineering-based studies and clinical practice." It was published in: 'State of Breastfeeding in the World' – Eds. Donovan SM, German JB, Lönnerdal B, Lucas A: "Human Milk: Composition, Clinical Benefits and Future Opportunities." Nestlé Nutr Inst Workshop Ser, vol 90, pp 13–32, (DOI: 10.1159/000490322 ) Nestlé Nutrition Institute, Switzerland/S. Karger AG., Basel, © 2019.
Historical imaging studies of breastfeeding (& bottle-feeding)
I have uploaded film sequences from three historical studies, each of which represents archival material, and which has not previously been available. While it may not be immediately clear what each one is showing, they represent a gateway into the original articles: Ardran et al, 1958a & b; Eishima, 1991; and Weber et al, 1986. Using three entirely separate methodologies (cine-X-ray; direct filming; 2D ultrasound) they all confirm the existence of peristaltic tongue movements as the obligate suckling action. Eishima's study shows that another element needs to be added to complete a more comprehensive 'Revised Suckling Physiology'; observatiosn which have since been confirmed for breastfeeding by Geddes et al, 2008. But, none of these studies are in conflict - instead they point the way forward to a more complete & synergistic model of infant suckling.
In three sections, immediately below, I have reproduced some dynamic film sequences from three historical imaging studies. These include: (i) the cineradiographic studies of breastfeeding and bottle-feeding, published by Ardran, Kemp & Lind in 1958; (ii) a study made by filming directly into the baby's oral cavity, through the back of a clear bottle teat - this study, conducted in 1988 was published in 1991; (iii) finally, there are two clips from our first ultrasound study (Weber et al, 1986) - they are of the same baby while both bottle-feeding and breastfeeding. I feel that, to a large extent, these early studies have been ignored - they use three different methodologes, yet each confirms that peristatlic tongue movements are omnipresent. These early findings were confirmed and ratified by our more recent ultrasound studies (further down this page). I am disconcerted by the efforts of one particular research group to try to deny the existence of peristaltic motion of the tongue, claiming instead that the baby relies predominantly on locally-generated, 'added' suction (cf NOT baseline suction) to extract milk from the breast. [Tracking ID: G-5X79KP6Q1X]
Cine-radiographic studies by Ardran, Kemp & Lind (1958b)
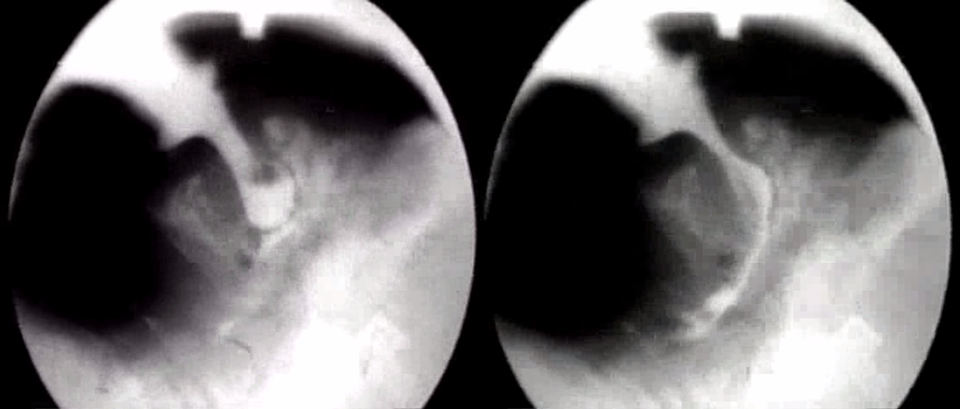
People have asked where the image above (from my Facebook page) comes from. So I'm posting archive videos of the ground-breaking research conducted by Dr Gordon Ardran (Oxford) and his colleagues F Kemp & J Lind (1958a & b). They made cine x-ray films of babies bottle-feeding and breastfeeding. Each of them comprises a four second exposure, looped so as to run continuously (i.e. the image repeats itself every 4 sec).
The bottle-feeding studies are easier to interpret (in terms of their imaging) as they were able to fill the bottle with barium milk. They also used an artifical lamb's teat - which was long and completely pliable.
The baby's tongue can clearly be seen indenting the teat, squeezing milk into the oral cavity. At two points, air bubbles can seen re-entering the teat from the baby's mouth - this indicates that as the baby removes milk from the bottle, suction builds up inside it, which is only relieved by air entering the teat, from the baby's mouth.
In the picture below, I've also uploaded a cine x-ray study of breast-feeding undertaken by Ardran, Kemp & Lind (1958a).
Unlike their bottle-feeding study, it is clearly NOT possible to fill the breast with barium milk! Instead, they have placed metallic discs on the breast surface, although there are no 'before' photos to show where these were located. They also coated the nipple with barium-opaque lanolin; at one point, the baby can be seen swallowing some of this!
In addition, the baby's body has to be moved away from the breast to create a good image; this means the baby is not ideally positioned for suckling and for removing milk effectively
It's not easy to see how far the breast enters the baby's mouth, but it certainly projects beyond that which is readily visible.
Direct filming of perstaltic tongue movements during bottle-feeding - Kazuko Eishima (1991)
Website for downloading paper: https://dokumen.tips/reader/f/the-analysis-of-sucking-behaviour-in-newborn-infants
In April 1988, Prof Kazuko Eishima on a sabbatical visit to Queen Charlotte's Hospital, London, undertook a novel research approach to studying the newborn's reflexes, under the auspices of David Harvey, Martin Richards, Deborah Rosenblatt, Heinz Prechtl and Bert Touwen.
She investigated the baby's feeding reflexes by filming directly into the baby's mouth, from behind a transparent bottle teat.
Key Summary points: (1) For anyone who doubts the existence of peristaltic tongue movements, I feel sure they will find this compelling - providing categorical proof of their existence.
(2) Eishima was the first researcher to observe, and to highlight, a localised drawing down of the rear of the tongue surface - this results in an exaggerated action, which clearly slows down overall suck duration. Her findings were later confirmed by Geddes et al (2008, & other later papers).
(3) She compared Non-Nutritive Sucking (NNS) on a blind teat, with Nutritive Sucking (NS) on two teats, one with a small hole (S) and one with a large hole (L). On the teat with the small hole, the normal peristaltic action seen during NNS was also observed, but with an exaggerated & prolonged tongue action. On the teat with a large hole, the baby only had a very loose grip on the teat (space around it in baby's mouth); with little effort it was swamped with fluid, while showing almost non-existent peristaltic tongue movements. On the teat with the small hole, sucking looks laboured, as if the baby is having to work hard to extract fluid - the inclusion of the 'added suction' elements would appear to endorse this view.
I have uploaded three segments from a film lasting 5min 55sec - Part 1 is 4min 4sec long, Part 2 - 56sec, & Part 3 - 53sec .
If you would like a transcript of the full narrative, please click on here to download a full narrative.
Original ultrasound studies of infant feeding - recorded 1984-5, published in 1986
The two videos (shown below) illustrate how relatively primitive ultrasound was in 1985; these videos being recorded on an ATL300. The same baby is shown in both videos, first feeding on a bottle, then on the breast.
On the bottle he seems to echo the words of Ardran et al (1958) who stated: “The various types of teat supplied for feeding babies were comparatively ineffective".
The bottle teat can be viewed as a static 'double echo' resting against the tongue - with both the inner and outer wall reflecting ultrasound. Throughout this sequence, the baby does not deform the teat bulb at all; it remains resistant to compression. The tongue only shows its usual rhythmic motion after it has passed the teat tip. At rest the baby shows a classical 'humped tongue', rising towards the roof of the mouth at the teat tip (this is similar in profile to the computer-generated 3D image of the tongue in Eishima's video).
As a consequence, this baby did not take any milk from the bottle - shown both by: the absence of swallows in this sequence; and the fast non-nutritive sucking rate.
Early ultrasound studies of infant feeding - recorded 1984-5, published in 1986
In stark contrast to the previous video, this baby swallows with every suck. A swallow is observed when the tissue at the back of the oral cavity, in the pharyngeal spce, move sharply up to disappear from view - then return a few frames later when the swalow is completed.
This sequence comprises 48 suck:swallows, in 5 bursts of 10, 11, 9, 10 & 9 suck/swallows in each burst. Swallows can be observed at the rear of the oral cavity (in perhaps the right hand 30-40% of the sector scan (image)). The tissues are clear in one frame, then disappear upwards, only to return a few frames later. When you can recognise them in this video, return to the bottle feeding one above, where you will see that swallows are absent.
Probable incidence of genuine low milk supply
As is well known, breast milk production is regulated by the process of 'supply-&-demand', so if there is inadequate 'demand' there will be inadequate 'supply'. Inadequate demand can take many forms, but crucially, perhaps the most important form is dependent on the baby's ability to access and remove synthesised milk. Any milk which is not removed will be interpeted by the breasts as 'not needed', will be re-absorbed, and milk supply down-regulated as a consequence. The down-regulation of milk supply in the first 4-6 weeks post-natally remains a largely unexplored, but potentially insidious cause of perceived breast milk insufficiency (PBMI); also referred to as self-reported insufficient milk (SRIM), Perez-Escamilla et al, 2019 (Click here for link to article).
The article attached was based on a Medical Research Council (MRC) funded research study aimed at investigating clinical problems of breastfeeding, specifically of low milk supply; it remains my best estimate of the probable incidence of insufficient milk supply in the general population, even though it is based on a professionally-referred clinical population.
Several issues need to be emphasised. First, because this was clinically-referred population of clients, several dedicated community healthcare professionals (M/ws, HVs, GPs) had already made a substantial input. As a consequence, 95% of referrals for low milk supply reported reliable, verifiable symptoms. Despite this, 85% of referrals for low milk supply were resolved by routine, higher-order recommendations - addressing the frequency or patterning of feeds; anatomical details of positioning and attachment; and by providing ongoing support and encouragement.
This leaves 15% of cases referred for low milk supply which were not routinely resolvable, and most will have necessitated given artificial formula to alleviate undersupply and poor infant growth. But within this 15% there were four distinct classes of problem, of which only two represent a biological predisposition to low milk supply, while two were avoidable and both should have, and could have, been avoided with more optimal management in the early days post-natally.
Of this 15%, only 1.3% represented a 'clinical patho-physiology' of the mother (or baby) which prevented an adequate milk supply being available. There was no duplication of any single entity, making it difficult to generalise from these cases. Nonetheless, milk intake was typically below 150g/24hr; in one case, being just 18ml for over 4 hours of suckling (the milk composition being normal, no elevated levels of any component, e.g. sodium). Clearly supplementation with formula is vital in such circumstances, but ALL mothers in this position continued to put their baby to the breast for whatever benefits they or their baby might achieve (immunity, fertility control, affectionate ties, closeness & reassurance of the infant). NB This group included one case of suspected Addison's Disease of the mother, and one case of Noonan's syndrome in the baby - neither of which represent a primary pathology of milk synthesis, on their own, but which is a secondary consequence of the primary condition.
Within the larger group, 4.6% of mothers suffered from genuine 'Physiological low milk supply', necessitating supplementation with formula to ensure adequate infant growth. In other words we were unable to boost supply in these mothers by routine technical advice; by changes to the patterning of feeds; by adjunctive pumping; and/or by use of pharmacological agents (under close supervision - including monitoring of maternal prolactin levels). Practically, these mother were producing between 150-350 g/24hr of breast milk, which falls below the 1st centile for milk supply (i.e. 'normal' for 1% of the population).
So, in summary, a total of 6% of cases referred for low milk supply (4.6%+1.3%) were proven as being real, and were unresolvable by routine measures. It is difficult to conceive of this percentage translating into a similar proportion of cases in the general population, so the probability of genuine low milk supply is likely to be under 5%.
There were two separate categories: 'Iatrogenic low milk supply' (2.6%) and 'Behavioural low milk supply' (2.6%), both of which do not represent physiological cases of low milk supply, but ones which have been acquired through the early mismanagement of breastfeeding. In such cases it appeared that there had been irreversible down-regulation of milk supply from an earlier higher level, but that once this had happened, it was not possible to reverse by routine methods. This also means that 5.2% of cases of low milk supply were the result of inappropriate management of breastfeeding in the early days (in contrast to the large number of mothers who were appropriately managed in the early days).
I leave others to speculate as to what represents the real incidence of genuine low milk supply in the overall population, but I firmly believe that estimates of 5-10% are wildy wrong - hence my claim that breastfeeding works for 98% of mothers (if correctly encouraged/managed).
Click here for link to pdf file
Breastfeeding and reverse 'nipple confusion'
Marina Rae (among others) asked about my views on whether the breast-fed baby can show 'nipple confusion' when confronted with bottles; in other words might it work in reverse. I wrote about this in 1995 for a presentation at the Pontifical Academic of Sciences, published as: Woolridge MW. Problems of establishing lactation. Special issue on Breast-feeding: Science and Society. Food & Nutrition Bulletin. 1996; 17: 316-23.
I have reproduced here the original pdf copy of my draft submission, with relevant sections highlighted in yellow and blue. This was written in 1995, so there have been several relevant publications since then. In 2000, we published 'Enabling Women to Breastfeed: A Review of Practices which Promote or Inhibit Breastfeeding - with Evidence-based Guidance for Practice', which reviewed research studies published up to that date; while the WHO/UNICEF published the 'Evidence for the Scientific Basis to the Ten Steps' in 1998 - https://www.ncbi.nlm.nih.gov/books/NBK153465/
The WHO/UNICEF Ten Steps have also been revised since then: https://www.who.int/nutrition/bfhi/ten-steps/en/
Over future months I plan to post pdf copies of my unpublished research manuscripts. These can be read online, but also downloaded (maybe for a small fee) - in addition, any embedded videos (e.g. ultrasound studies) will be downloadable as educational resources.